A definitive celiac disease diagnosis typically requires a specific celiac disease blood test followed by an endoscopic biopsy. The process begins with a serology panel screening for tTG-IgA antibodies. If positive, a gastroenterologist performs an upper endoscopy to identify villous atrophy in the small intestine, confirming the autoimmune reaction to gluten.
Navigating the path to a celiac disease diagnosis can be confusing, often involving a mix of vague symptoms, dietary experimentation, and medical terminology. However, establishing a clinical diagnosis is critical for long-term health management. Unlike non-celiac gluten sensitivity, celiac disease is an autoimmune condition where the ingestion of gluten damages the small intestine. Therefore, relying on guesswork is not an option. Medical professionals follow a strict protocol involving serology (blood tests) and histology (biopsy) to confirm the disease.
Why You Must Keep Eating Gluten Before Testing
Before diving into the specifics of the celiac disease blood test and biopsy, there is one critical rule that every patient must follow: do not stop eating gluten before you have been tested.
This is the most common mistake patients make. When you experience chronic bloating, fatigue, or digestive distress, the natural instinct is to eliminate the suspected trigger immediately. However, diagnostic tests for celiac disease rely on the presence of an active autoimmune reaction. The blood tests look for specific antibodies produced by the immune system in response to gluten, and the biopsy looks for physical damage (villous atrophy) caused by that reaction.
If you remove gluten from your diet prior to testing, your antibody levels may drop to undetectable ranges, and your intestinal lining may begin to heal. This can lead to a “false negative” result, leaving you without a diagnosis and potentially causing future medical complications.
The Recommended “Gluten Challenge”
If you have already adopted a gluten-free diet but need a confirmed diagnosis, physicians will prescribe a “gluten challenge.” This typically involves:
- Duration: Reintroducing gluten for at least 6 to 8 weeks prior to the blood test and biopsy.
- Quantity: Consuming the equivalent of two slices of wheat bread (approximately 3–10 grams of gluten) every single day.
While this reintroduction can be uncomfortable for those with active disease, it is the only way to ensure the celiac disease blood test and biopsy yield accurate data.

Serology Panels (tTG-IgA): The Screening Phase
The diagnostic journey almost always begins with a blood draw. Serologic tests screen for antibodies that are elevated in people with untreated celiac disease. These tests are highly sensitive and specific, but they must be interpreted correctly.
Tissue Transglutaminase IgA (tTG-IgA)
The tTG-IgA test is widely considered the primary screening tool for celiac disease. Tissue transglutaminase (tTG) is an enzyme in the intestine. In celiac patients, the immune system mistakenly attacks this enzyme when gluten is present.
- Sensitivity: Approximately 95-98% of celiac patients will test positive.
- Specificity: It rarely yields a positive result in people who do not have celiac disease.
Because it is the most effective marker, it is usually the first test ordered. However, for the test to be accurate, the patient must have normal levels of total IgA.
Total IgA
A comprehensive celiac panel must include a Total IgA measurement. IgA (Immunoglobulin A) is a type of antibody. Approximately 2-3% of people with celiac disease have a condition called selective IgA deficiency. If a patient is IgA deficient, the standard tTG-IgA test will produce a false negative because the patient cannot produce enough IgA antibodies to trigger a positive result, regardless of whether they have celiac disease.
If a Total IgA deficiency is found, doctors will switch to IgG-based tests (such as tTG-IgG or DGP-IgG) to ensure accuracy.
Deamidated Gliadin Peptide (DGP)
DGP tests (IgA and IgG) are often used as secondary markers. They are particularly useful in children under the age of two, as the tTG levels in very young children may not yet be elevated enough for detection. They are also utilized for patients with IgA deficiency.
Endomysial Antibody (EMA)
The EMA-IgA test is highly specific—even more so than the tTG-IgA—but it is less sensitive and more expensive to run. It is often used as a tie-breaker or confirmatory blood test when the tTG-IgA results are borderline.

The Gold Standard: Endoscopy and Biopsy
While serology provides strong evidence, the celiac disease blood test and biopsy generally go hand-in-hand for a confirmed diagnosis in adults. The upper endoscopy (EGD) with small intestinal biopsy remains the “gold standard” for diagnosis.
The Procedure
During an upper endoscopy, a gastroenterologist guides a thin, flexible tube with a camera (endoscope) through the mouth and into the small intestine. The patient is typically sedated and feels no pain. The doctor examines the duodenum (the upper part of the small intestine) for visible signs of inflammation, scalloping, or fissuring.
Crucially, the doctor will take multiple tissue samples (biopsies) from different sections of the duodenum. This is necessary because celiac damage can be patchy; one area might be damaged while a neighboring area appears normal.
Understanding the Marsh Classification
Pathologists examine the biopsy samples under a microscope and grade the damage using the Marsh Classification System. This score determines the severity of the disease:
- Marsh 0: Normal mucosa. No celiac disease.
- Marsh 1 (Infiltrative): Normal villi architecture but an increased number of intraepithelial lymphocytes (immune cells). This is non-specific and can be seen in other conditions.
- Marsh 2 (Hyperplastic): Enlarged crypts (grooves between villi) and increased immune cells, but villi are not yet flattened.
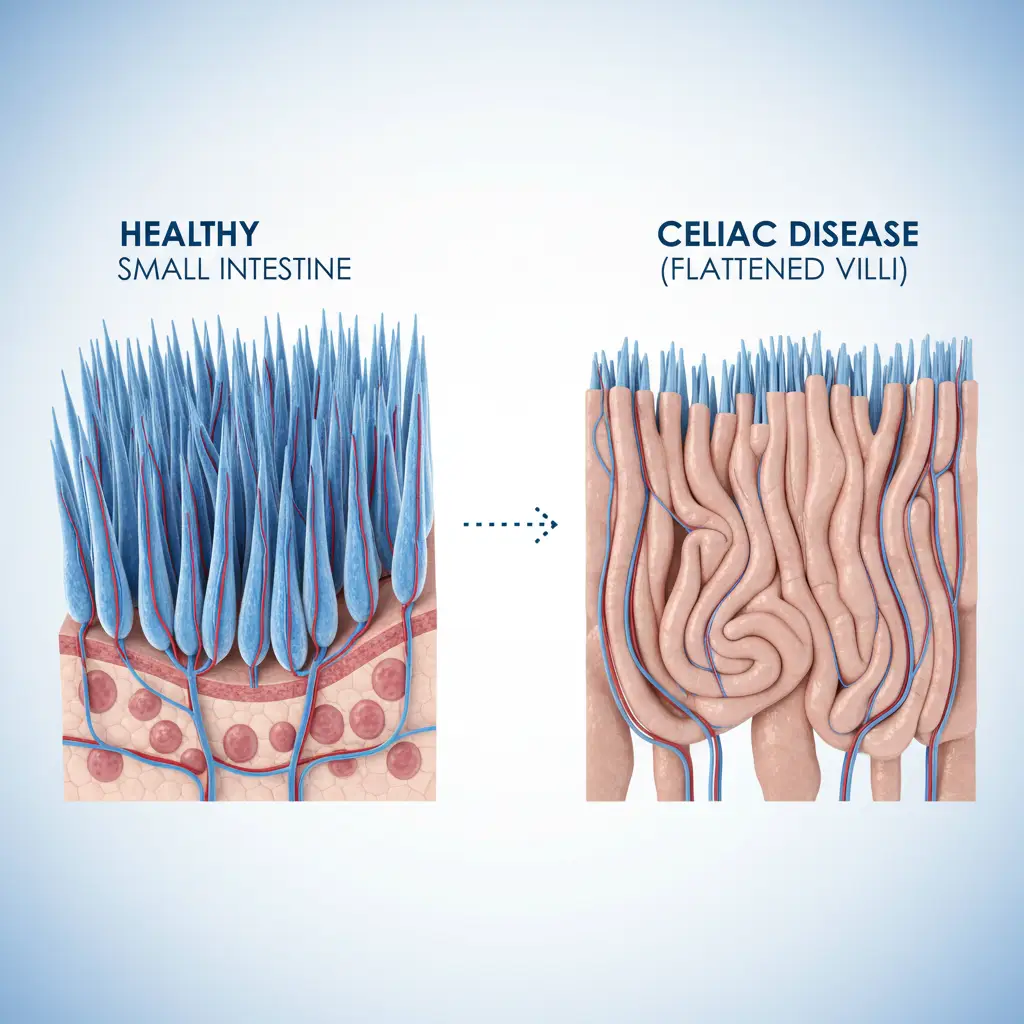
- Marsh 3 (Destructive): The hallmark of celiac disease. This stage involves villous atrophy (flattening of the finger-like projections that absorb nutrients). It is subdivided into:
- 3a: Partial villous atrophy.
- 3b: Subtotal villous atrophy.
- 3c: Total villous atrophy (completely flat).
A Marsh 3 score, combined with positive serology, confirms the diagnosis of celiac disease.
Genetic Testing (HLA-DQ2/DQ8)
Genetic testing is a valuable tool, but it functions differently than the celiac disease blood test and biopsy. It does not diagnose active disease; rather, it assesses the potential to develop the disease.
The Role of HLA-DQ2 and HLA-DQ8
Celiac disease is hereditary. To develop the condition, a person must carry specific genetic variants of the Human Leukocyte Antigen (HLA) complex, specifically HLA-DQ2 or HLA-DQ8.
- The “Rule-Out” Value: If a patient does not carry either of these gene variants, it is virtually impossible for them to develop celiac disease. Therefore, a negative genetic test effectively rules out the condition for life (negative predictive value >99%).
- The Limitation: Approximately 30-40% of the general population carries these genes, but only 1% of the population develops celiac disease. Therefore, a positive genetic test does not mean you have celiac disease; it only means you are genetically susceptible.
When is Genetic Testing Used?
Doctors typically order genetic testing in specific scenarios where serology or biopsy results are ambiguous:
- Equivocal Results: When blood tests and biopsies do not align (e.g., positive blood test but negative biopsy).
- Already Gluten-Free: If a patient has been on a gluten-free diet for a long time and refuses to do a gluten challenge, a genetic test can determine if celiac disease is even a possibility. If negative, they don’t need to challenge. If positive, a challenge is necessary for confirmation.
- Family Screening: To assess the risk for first-degree relatives of a diagnosed celiac patient.

Navigating Diagnostic Challenges
Seronegative Celiac Disease
In rare cases, a patient may have severe villous atrophy (Marsh 3) appearing on a biopsy, yet their blood tests (tTG-IgA) are negative. This is known as seronegative celiac disease. This creates a diagnostic dilemma and often requires ruling out other causes of villous atrophy, such as medications (olmesartan), Giardia infection, or other autoimmune enteropathies.
Pediatric Diagnosis Without Biopsy?
Recent guidelines from the European Society for Paediatric Gastroenterology Hepatology and Nutrition (ESPGHAN) suggest that in certain pediatric cases, a biopsy may be avoided. If a child has tTG-IgA levels more than 10 times the upper limit of normal, a positive EMA test, and compatible symptoms, a diagnosis might be made based on serology alone. However, this “no-biopsy” approach is strictly regulated and typically does not apply to adults.
People Also Ask
Can celiac disease be diagnosed without a biopsy?
In adults, a biopsy is still considered the gold standard and is rarely skipped. In children, strict criteria (very high antibody levels) may allow for a diagnosis without biopsy, but this decision must be made by a pediatric gastroenterologist. For most, the biopsy is essential to confirm the extent of damage and rule out other conditions.
How long does it take to get celiac biopsy results?
After the endoscopy, the tissue samples are sent to a pathology lab. It typically takes 3 to 7 days for the pathologist to stain, examine, and grade the samples (Marsh classification) and send the report back to your doctor.
Can a blood test be wrong about celiac disease?
Yes. False negatives can occur if the patient is IgA deficient or has not been eating enough gluten (the most common cause). False positives are rarer but can happen in patients with other autoimmune disorders (like Type 1 Diabetes) or liver disease, which is why a biopsy is required for confirmation.
Is there a home test for celiac disease?
There are at-home screening kits that test for tTG-IgA antibodies using a finger-prick blood sample. While these can indicate a possibility of celiac disease, they are not diagnostic. A positive home test must always be followed up with a professional venous blood draw and a confirmatory biopsy by a specialist.
What is the difference between gluten sensitivity and celiac testing?
There is currently no validated biomarker or test for Non-Celiac Gluten Sensitivity (NCGS). NCGS is a diagnosis of exclusion, meaning you must first test negative for celiac disease (via blood and biopsy) and wheat allergy before being diagnosed with sensitivity based on symptom relief.
Do I need to undergo a biopsy if I have the genes?
Having the genes (HLA-DQ2 or HLA-DQ8) does not mean you have celiac disease; it only means you are at risk. You do not need a biopsy solely based on genetics. A biopsy is only indicated if you also have elevated antibodies or persistent symptoms suggesting active disease.