The primary difference between celiac disease and gluten intolerance lies in the underlying biological mechanism. Celiac disease is a genetic autoimmune disorder where gluten ingestion damages the small intestine’s villi. Conversely, gluten intolerance (Non-Celiac Gluten Sensitivity) triggers digestive and extra-intestinal symptoms without causing tissue damage or an autoimmune response, while wheat allergy is an IgE-mediated allergic reaction specifically to wheat proteins.
Navigating the landscape of gluten-related disorders can be confusing. Many individuals experience discomfort after consuming bread or pasta, yet the root cause varies significantly between patients. Understanding the specific medical distinctions between Celiac Disease (CD), Non-Celiac Gluten Sensitivity (NCGS), and Wheat Allergy is critical, as the long-term health implications and management strategies differ drastically for each condition.
The Core Distinctions: Autoimmune vs. Innate Response
To accurately determine the difference between celiac and gluten intolerance, one must look at the immune system’s involvement. While all three conditions involve a reaction to wheat or gluten, the biological pathways are distinct.
Autoimmune vs. Allergic vs. Innate
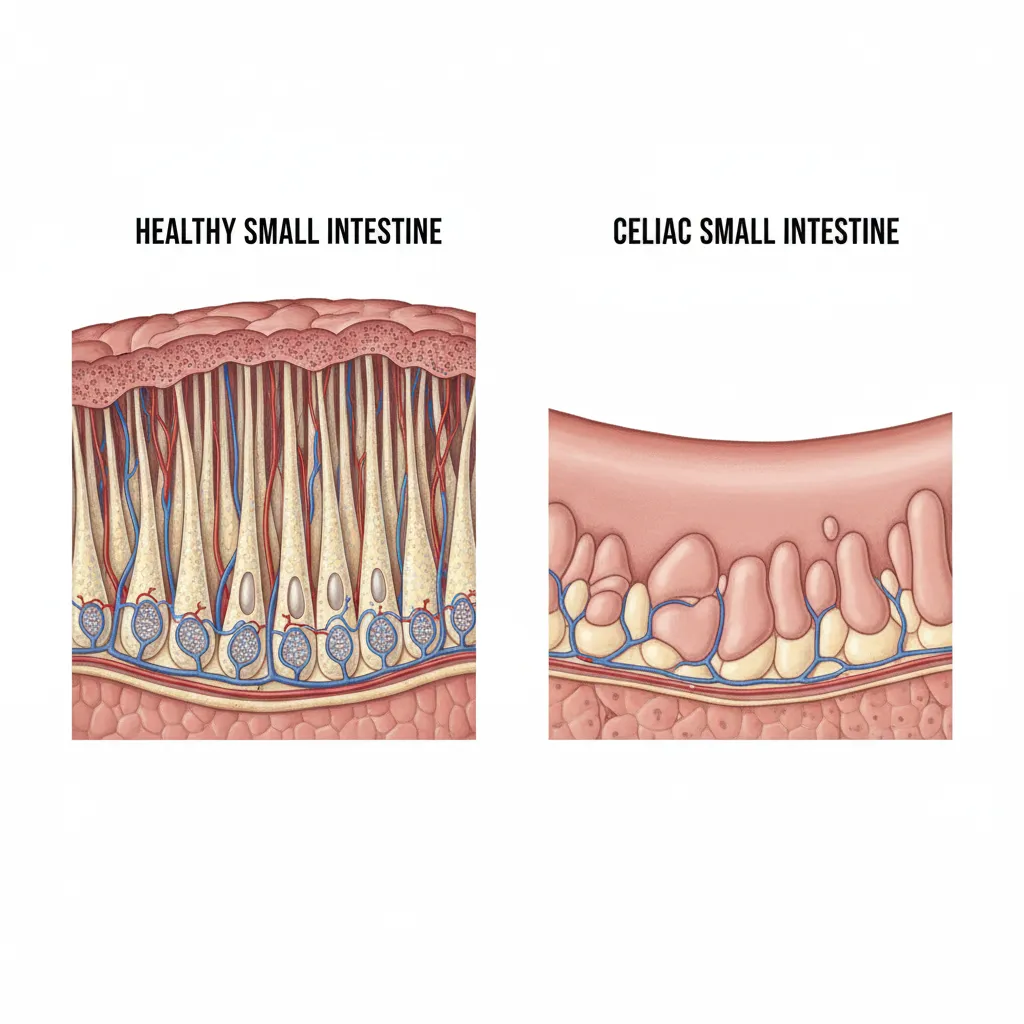
Celiac Disease is an autoimmune condition. When a person with celiac disease ingests gluten (a protein found in wheat, barley, and rye), their immune system launches an attack on the small intestine. This is not merely an intolerance; it is a self-destructive immune response mediated by T-cells that leads to villous atrophy—the flattening of the nutrient-absorbing finger-like projections in the gut.
Wheat Allergy, by contrast, is a classic type I hypersensitivity reaction. It is mediated by IgE antibodies. Upon exposure to wheat proteins (which may or may not include gluten), the body releases histamine and other chemicals, causing immediate reactions ranging from hives to anaphylaxis.
Non-Celiac Gluten Sensitivity (NCGS), often referred to as gluten intolerance, is believed to involve the innate immune system but lacks the specific antibodies (tTG-IgA) and intestinal damage seen in celiac disease. It is a diagnosis of exclusion, meaning it is identified only after celiac disease and wheat allergy have been ruled out.
Understanding Celiac Disease: The Autoimmune Threat
Celiac disease is a serious, lifelong genetic disorder affecting approximately 1% of the global population. It is triggered by the ingestion of gluten in genetically predisposed individuals, specifically those carrying the HLA-DQ2 or HLA-DQ8 genes.
The Pathophysiology of Damage
When gluten reaches the small intestine of a celiac patient, the enzyme tissue transglutaminase (tTG) modifies the gluten peptides. The immune system mistakenly identifies these modified peptides as foreign invaders. The resulting immune attack causes chronic inflammation and damages the villi. This damage inhibits the body’s ability to absorb vital nutrients, leading to malabsorption.
Long-term Health Risks
If left undiagnosed or untreated, the difference between celiac and gluten intolerance becomes dangerous. While intolerance causes discomfort, untreated celiac disease can lead to:
- Iron deficiency anemia that does not respond to supplementation.
- Early-onset osteoporosis or osteopenia.
- Infertility and miscarriage.
- Neurological conditions like migraines and neuropathy.
- Increased risk of intestinal lymphomas (cancer).

Non-Celiac Gluten Sensitivity (NCGS) Explained
Non-Celiac Gluten Sensitivity (NCGS) is the clinical term for what many people call “gluten intolerance.” Patients with NCGS experience symptoms similar to celiac disease upon consuming gluten, yet they test negative for celiac antibodies and show no signs of intestinal damage on biopsy.
The “FODMAP” Factor
Recent research suggests that for some individuals diagnosed with NCGS, the culprit may not be gluten at all, but rather Fructans—a type of fermentable carbohydrate found in wheat. This falls under the category of FODMAPs (Fermentable Oligosaccharides, Disaccharides, Monosaccharides, and Polyols). These carbohydrates can cause significant bloating and gas in people with Irritable Bowel Syndrome (IBS), complicating the diagnosis.
Symptoms of NCGS
The symptoms of NCGS can be intestinal and extra-intestinal, often appearing hours to days after ingestion:
- Digestive: Bloating, abdominal pain, diarrhea, and constipation.
- Neurological: “Brain fog,” headache, and fatigue are reported significantly more often in NCGS than in classic celiac presentations.
- Musculoskeletal: Joint pain and numbness in extremities.
Wheat Allergy Mechanisms
A wheat allergy is fundamentally different from both celiac disease and NCGS. It is more common in children and is often outgrown, though adults can develop it as well. It is strictly an immune reaction to one of the many proteins found in wheat, such as albumin, globulin, gliadin, or glutenin.
The Immediate Reaction
Unlike celiac disease, which can take days or weeks to manifest symptoms, a wheat allergy reaction usually occurs within minutes to hours of consumption. The body produces specific IgE antibodies to fight the wheat protein.
Symptoms include:
- Swelling, itching, or irritation of the mouth or throat.
- Hives, itchy rash, or swelling of the skin.
- Nasal congestion.
- Difficulty breathing (Asthma-like symptoms).
- Anaphylaxis (a life-threatening reaction requiring epinephrine).

Symptom Overlap and Comparison
The diagnostic challenge lies in the massive overlap of symptoms. A patient complaining of bloating and fatigue could fit into any of the three categories. However, the nuance often lies in the timing and the extra-intestinal manifestations.
Comparison Matrix
- Onset of Symptoms:
- Wheat Allergy: Minutes to hours.
- NCGS: Hours to days.
- Celiac Disease: Days to weeks (chronic accumulation), though some react acutely.
- Systemic Impact:
- Wheat Allergy: Respiratory and dermatological focus.
- NCGS: Neurological (brain fog) and digestive focus.
- Celiac Disease: Malabsorption and autoimmune focus (anemia, bone density).
- Damage:
- Wheat Allergy: No permanent organ damage.
- NCGS: No permanent organ damage observed.
- Celiac Disease: Permanent intestinal atrophy if gluten is continued.
Differential Diagnosis: Testing and Screening
Determining the difference between celiac and gluten intolerance requires a strict medical protocol. Self-diagnosis is highly discouraged because the treatments differ significantly.
Blood Panels (Serology)
The first step is usually a blood test. Doctors look for elevated levels of certain antibodies:
- Tissue Transglutaminase IgA (tTG-IgA): The most sensitive and specific screening test for celiac disease.
- Total IgA: Used to ensure the patient doesn’t have an IgA deficiency, which would make the tTG test invalid.
- IgE Testing: Used to screen for Wheat Allergy.
Endoscopy and Biopsy
If blood tests are positive for celiac antibodies, the “gold standard” for diagnosis is an upper endoscopy. A gastroenterologist takes small tissue samples from the small intestine to check for villous atrophy. In NCGS, this biopsy will appear normal (Marsh 0 score), whereas in celiac disease, it will show varying degrees of damage (Marsh 3 score).
The Elimination Diet Protocol
If celiac disease and wheat allergy are ruled out via testing, but symptoms persist, a diagnosis of NCGS is considered. This is confirmed through an elimination diet followed by a monitored reintroduction of gluten (often double-blinded in clinical settings) to see if symptoms return.

Management and Lifestyle Strategies
Once a diagnosis is secured, the management path diverges. Understanding the difference between celiac and gluten intolerance dictates how strict your lifestyle must be.
Celiac Disease: Zero Tolerance
For celiac patients, the diet must be strict and lifelong. Even microscopic amounts of gluten (crumbs in a toaster, shared pasta water) can trigger an autoimmune reaction and intestinal damage. Cross-contamination is a major concern. Celiac patients typically require separate cookware and dedicated gluten-free preparation areas.
NCGS: Threshold Tolerance
Management for NCGS is often less rigid. Many individuals with gluten intolerance can handle small traces of gluten or cross-contamination without severe symptoms. The goal is symptom management rather than preventing autoimmune damage. Some patients find they can reintroduce sourdough bread or ancient grains over time.
Wheat Allergy: Specific Avoidance
Those with a wheat allergy must avoid wheat in all forms but may be able to safely consume barley and rye (which contain gluten but not wheat proteins). However, because wheat is a top allergen, they must be vigilant about carrying epinephrine auto-injectors if they have a history of anaphylaxis.
In summary, while the symptoms may feel similar, the biological reality of these conditions varies immensely. Whether you are dealing with the autoimmune destruction of celiac disease, the histamine response of an allergy, or the inflammatory discomfort of sensitivity, obtaining a correct diagnosis is the first step toward reclaiming your health.
Can you have celiac symptoms but test negative?
Yes, this is possible but rare. It is known as seronegative celiac disease. It can occur if you have an IgA deficiency, if you were already on a gluten-free diet before testing, or in rare cases where the immune reaction is localized to the intestine but not present in the blood. An endoscopy is usually required to confirm this diagnosis.
Is gluten intolerance the same as wheat allergy?
No. Gluten intolerance (NCGS) is a digestive and systemic sensitivity to gluten without an allergic immune response. Wheat allergy is an IgE-mediated immune reaction specifically to wheat proteins, which can cause hives, swelling, and anaphylaxis, distinct from the digestive distress of intolerance.
Will cutting out gluten help if I don’t have celiac?
If you have Non-Celiac Gluten Sensitivity (NCGS), cutting out gluten will alleviate your symptoms. However, if your symptoms are caused by other factors like IBS or FODMAP sensitivity, removing gluten alone might not solve the issue. It is best to consult a dietitian.
What is the gold standard for diagnosing celiac disease?
The gold standard for diagnosing celiac disease is a duodenal biopsy performed during an upper endoscopy. This allows the gastroenterologist to visually examine the small intestine and analyze tissue samples for the characteristic villous atrophy caused by the autoimmune response.
Can gluten sensitivity turn into celiac disease?
Currently, there is no medical evidence to suggest that Non-Celiac Gluten Sensitivity turns into celiac disease. They are considered separate conditions with different biological mechanisms. However, a person could be misdiagnosed with sensitivity when they actually have early-stage celiac disease.
What are the silent symptoms of celiac disease?
“Silent” or asymptomatic celiac disease occurs when patients have intestinal damage but no digestive symptoms. However, they may present with non-digestive signs such as unexplained anemia, dental enamel defects, osteoporosis, infertility, or varying degrees of fatigue.